Aortic valve reconstruction
The purpose of aortic valve reconstruction is to repair the patient's own aortic valve in such a way as to restore it to its full function. This is a highly complex surgical procedure, which can provide a useful alternative to using prosthetic aortic valves.

Restoring a dilated aortic valve to its full function is a complex surgical procedure. A successful procedure results in the preservation of the patient's own valve. This means the patient does not require anticoagulant medication (or, more precisely, anticoagulant treatment using the vitamin K antagonist coumarin; Falithrom™ / Marcumar™ [phenprocoumon]) for life. The issue of wear and tear that is associated with prosthetic tissue valves also does not apply to this procedure.
Over the past 15 years, two standard techniques have emerged, both of which were named after the people responsible for their development and introduction, Sir Magdi Yacoub (London, England) and Tirone David (Toronto, Canada). These techniques have since been expanded upon, and other, simpler techniques have been developed, so much so that today's heart surgeons can choose from a whole range of techniques at their disposal. This allows them to tailor the process of reconstructing the aortic valve to the exact requirements of the individual patient. In light of this, the procedures developed by Yacoub and David should no longer be regarded as representing competing techniques. Instead, they should be seen as offering patient-oriented solutions, with selection depending on the tissue morphology of the individual patient's heart valve. These procedures are further complemented by additional techniques aimed at ensuring optimal valve function and improved durability. In patients who only have minor changes to the heart valves, surgeons also have the option of choosing simplified procedures, which also pose a lower risk to the patients.
As a rule, valve reconstruction is only possible in patients whose aortic valve is dilated, but whose aortic valve leaflets (cusps) have a normal structure and shape. In rare cases, valve reconstruction may be possible in patients who present with what is referred to as "bicuspid valves", a congenital abnormality that results in the aortic valve having two instead of three valve leaflets.




Depending on the severity of the aortic valve defect present, patients very often present with an aortic aneurysm (enlargement of the aorta), which will also need to be treated using these procedures. These techniques therefore fulfill another therapeutic purpose: not only do they prevent an aortic aneurysm from rupturing, but they also prevent the fatal consequences so frequently associated with the rupture of an aneurysm.
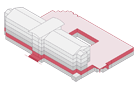
Changes to the aortic valve, which is situated at the very base of the aorta (aortic root), are usually the result of an enlargement of the aorta (aortic aneurysm). There are two different sections of the aorta that, when affected by aneurysms, can lead to the aortic valve no longer being able to close properly.
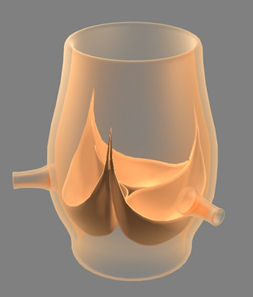
An isolated dilation affecting the aorta at the level of the commissures, combined with an aneurysm in the sinuses, can be repaired using the Yacoub procedure, by remodeling the aortic wall in the affected area and to stabilizing the commissures.

If the dilated area extends across both levels, the valve should be replaced using the David reimplantation procedure.

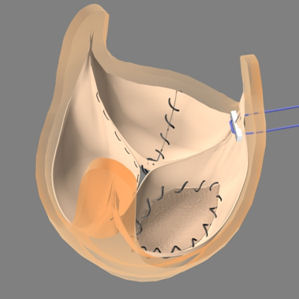

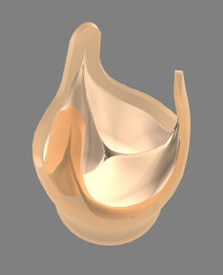
The use of suitable techniques allows the optimization of cusp function. The most commonly used technique is the Trussler stich. Following resuspension, the cusps are plicated, which tightens and lifts the edges to achieve improved coaptation.
Remodeling of the cusps can also be achieved by using patch enlargement, which involves plication of the free edge of the cusp, or removal of sections of the cusp to reduce its overall size.
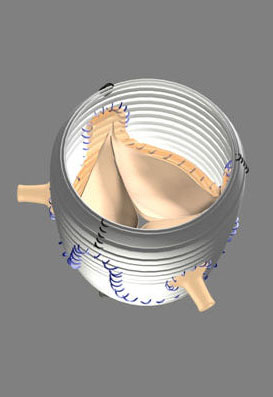
Although remodeling and resuspension already constitute a highly complex technique, the procedure is not completed until after coronary artery reimplantation. All of this makes for a time-consuming and demanding procedure, which requires considerable amounts of surgical expertise. As a matter of fact, only a small number of cardiac surgeons in Germany perform this type of surgery by following these highly complex procedures.
The surgical procedure can be simplified by using what is referred to as a supra-coronary prosthesis to simply re-attach commissures that are misaligned or separated (resuspension). Not only does this method eliminate the need for complex reconstruction of the aortic valve, it also eliminates the need for reimplantation of the coronary arteries, an extremely time-consuming procedure.
The process of attaching the prosthesis to the aorta (following remodeling, reimplantation or resuspension) can take place once the aorta has been clamped, or hypothermic circulatory arrest has been induced. Depending on the length of the aortic aneurysm involved, the prosthesis can then be attached to the aortic arch, or secured inside of the aortic arch. Complete removal of all diseased tissue from the aneurysm is essential for the long-term prevention of further aneurysms.
Surgical results
In terms of long-term results, aortic valve reconstruction has to be able to compete with heart valve replacement. In fact, in terms of perioperative risk (risk of complications during or after surgery), an international comparison of data shows that this type of surgery, when performed by experienced surgeons, carries no more risk than aortic valve replacement surgery or surgery to replace the aorta. The risk of premature mortality is between 5-8% for this type of surgery.
Furthermore, it is important to mention that the durability of reconstruction surgery compares favorably with that of valve replacement surgery. The percentage of patients who require further valve replacement surgery as a result of leakiness or narrowing after surgery, in order to replace the valve and aorta with a valved conduit (tube-shaped prosthesis with mechanical valve), is extremely low. In fact, the long-term risk is lower than 5%. Patients whose valves are replaced with mechanical valves will, of course, need to take coumarin for life.
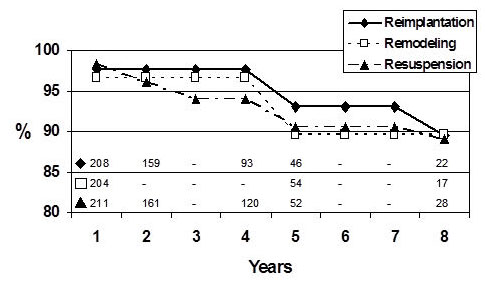
International data on valve reconstruction show that valve function remains good even after many years. The quality of valve function following surgery is assessed by freedom from reoperation, i.e. the number of patients not requiring repeat valve surgery as a result of renewed dilation or leakiness. Based on currently available results for the past 8-10 years, all three procedures appear to produce similar results for the first 5 years following surgery. Beyond 5 years, the David procedure (reimplantation) appears to perform slightly better, showing slightly superior stability for up to 8 years following surgery. One point to remember with regard to all reconstruction methods is that patients who have undergone these procedures (and who do not have other indications for coumarin therapy) do not have to take anticoagulant medication.
Summary
The techniques used as part of aortic reconstruction surgery are highly complex, requiring a high level of skill and expertise from individual surgeons. Not all German centers are capable of performing these procedures successfully. Successful reconstruction surgery results in a valve that functions perfectly for many years. Successful reconstruction surgery can therefore go a long way towards preserving a patient's quality of life, by eliminating the need for life-long anticoagulant medication. Based on currently available results for the past 8-10 years, properly reconstructed valves can be expected to remain stable over long periods of time. Future studies may provide even more convincing data on the superiority of the David procedure and the long-term stability of its results. Given the complexity of the condition being treated, however, both an in-depth consultation with the patient and an individualized surgical approach remain absolutely essential.
Source:
Albes JM, Stock UA, Hartrumpf M
Restitution of the aortic valve: what is new, what is proven, and what is obsolete? Ann Thorac Surg 2005;80:1540-9