Mitral valve reconstruction
This type of surgery restores valve function while also preserving the patient's own valve. In contrast to valve replacement surgery, this type of surgery does not require follow-up treatment with anticoagulant medication.

Mitral valve reconstruction
The past 12 years have seen a significant increase in mitral valve surgery. There has been a marked increase in the number of patients undergoing mitral valve reconstruction, i.e. surgery to restore valve function while preserving the patient's own valve. For the past three years now, more patients have undergone valve reconstruction surgery than valve replacement surgery. Isolated mitral valve defects are increasingly being treated using minimally-invasive procedures.
The benefits of this are obvious: Successful repair restores the natural valve's function, while avoiding the need for anticoagulant medication such as Marcumar™ or Falithrom™ [phenprocoumon].
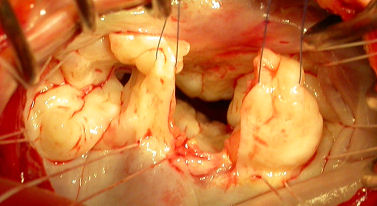
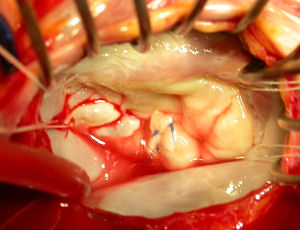
A successful procedure that restores mitral valve function demands a detailed knowledge of the different components the mitral valve.

Mitral valve function is based on 4 valve components
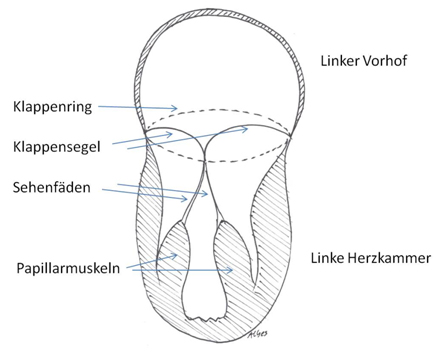
- Both leaflets (which resemble a bishop's mitre, or "mitra")
- The attachments of the leaflets inside the valve's annulus
- The fibrous tendons (chordae tendineae)
- The papillary muscles
These four components have to work in harmony if the mitral valve is to open and close properly.
Repair is only possible if neither the annulus, valve leaflets, fibrous tendons or papillary muscles show any severe tissue changes, e.g. as a result of calcification or severe tissue thickening. Typically, reconstruction is only possible in cases that involve an enlargement of the valve apparatus, which results in the valve not closing properly (regurgitation).
Although pathological changes to any of these components will result in the disruption of normal valve closure, a number of components may be affected. A whole range of techniques are available that can restore individual components to their normal function.
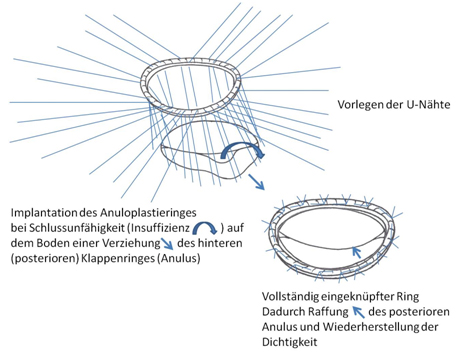
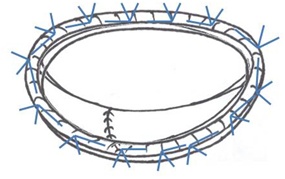
Annuloplasty
The shape and size of the annulus can be stabilized using a pre-shaped ring made of synthetic materials.
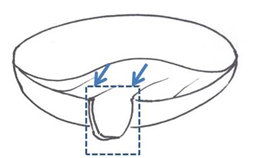
Leaflet reconstruction
The valve leaflets can be tightened, reduced in size, or enlarged.
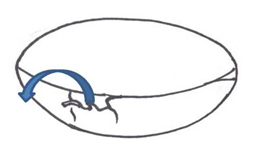
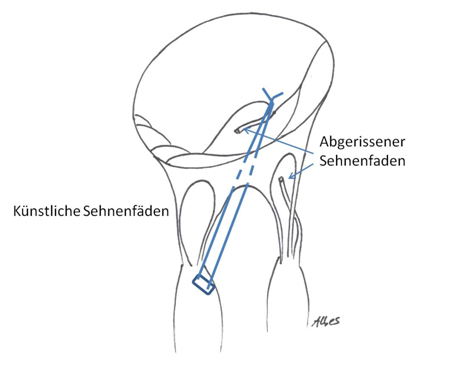
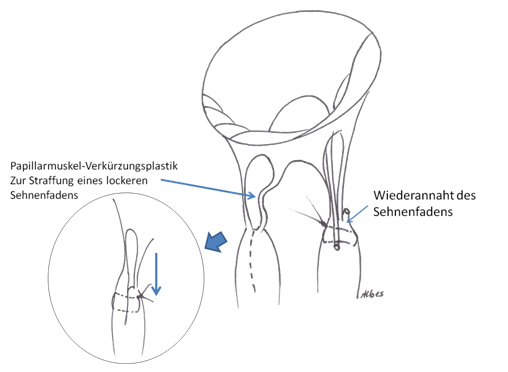
Chordal replacement / transposition
The chordae tendineae can be tightened, transposed, stretched or replaced/reinforced with artificial chords.
Papillary muscle shortening / transposition
The papillary muscles can be shortened or transposed. Their function, however, which is reminiscent of a parachutist actively pulling on the chords of a parachute, cannot be restored.
In an ideal case scenario, and even when different parts of the valve are severely affected, reconstruction can achieve results close to restoring normal function. However, a valve can only be restored to its full function in cases involving very minor, clearly defined changes.
A diagnostic assessment using cardiac catheterization and echocardiography prior to surgery makes it possible to determine with certainty whether reconstruction is feasible. The final decision, however, can only be taken in the operating room, when the surgeon is able to examine the actual valve and perform tests to establish how well its components are functioning. This type of procedure can only be performed by a highly experienced surgeon, who is able to determine during surgery whether valve repair is likely to result in adequate valve function being restored. If valve repair is unlikely to restore adequate valve function, the procedure is neither viable nor advisable and, if this is the case, valve replacement surgery is the safer alternative.
All of these procedures can be combined as required in order to ensure adequate restoration of the valve and its function.
Description of individual procedures
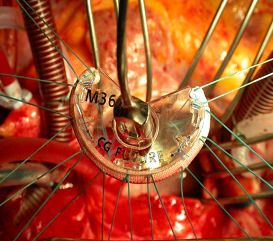
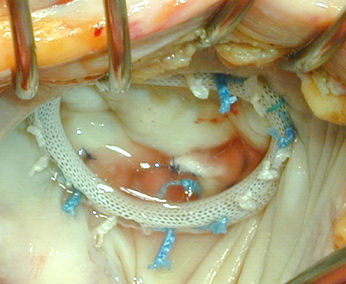
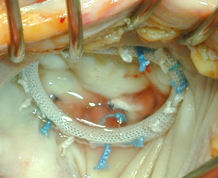
Annuloplasty using annuloplasty rings
Manufacturers have made a vast number of different annuloplasty rings available: there are rigid, semi-rigid and flexible, as well as closed, open and partial rings. The materials used also differ widely. One thing they all have in common, however, is that they have to be made of non-degradable materials, so that the patient's tissue has to grow around them. This of course means that while the natural valve leaflets and their function are preserved, some synthetic material remains inside the body long-term. This does not present a problem, as long as the patient ensures that they take antibiotics for any infections that might result in bacteria getting into the blood stream (this is referred to as prophylaxis against infective endocarditis).
Leaflet reconstruction
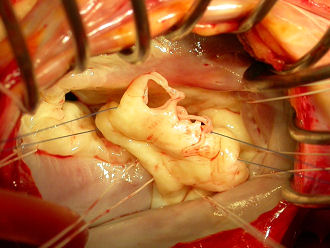


Repair of the chordae tendineae and papillary muscles
A typical form of mitral valve repair consists of the surgical correction of the posterior valve leaflet using quadrangular resectioning, followed by the stabilization of the annulus with an artificial annuloplasty ring.

Survival rates
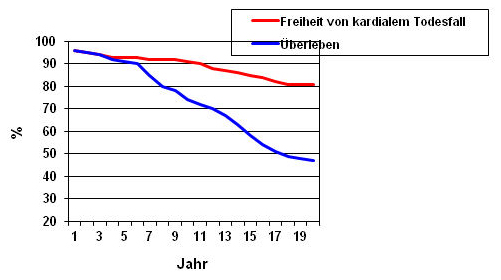
In most cases, long-term results are good. 70% of patients are still alive 10 years after surgery (blue curve).
Reoperation rates
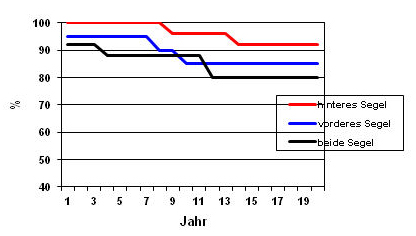
The quality of the initial treatment is not the only reason for why a patient might require reoperation. This also depends on the degree of initial damage affecting the valve leaflets. I particular, reconstruction of the posterior valve leaflet shows excellent long-term results. Even after 20 years, reconstructed valves still function perfectly in 90% of patients.
Minimally-invasive mitral valve surgery
Mitral valve surgery can also be performed using minimally-invasive techniques. Even minimally-invasive procedures, however, require the use of cardiopulmonary bypass (a heart-lung machine), which is connected via the blood vessels in the groin. Access to the heart is via a small incision in the right side of the chest. As other sections of the heart cannot be reached, this type of surgery is only suitable in patients with isolated mitral valve defects. As with open surgery, this technique is suitable for both valve reconstruction and valve replacement. However, it cannot be used in patients who have developed adhesions in the chest following surgery or radiation therapy. In spite of this, Germany has seen a steady increase in the number of patients with isolated mitral valve defects being treated with minimally-invasive procedures.