Aortic prosthetic reconstruction
Prosthetic reconstruction is used in patients whose aneurysms are of a considerable size. Large aortic aneurysms are at risk of dissection or rupture, both of which constitute life-threatening situations. Depending on the exact diagnosis, an aortic prosthesis is implanted using either open surgery or catheter-based procedures.

What is an aortic prosthesis?
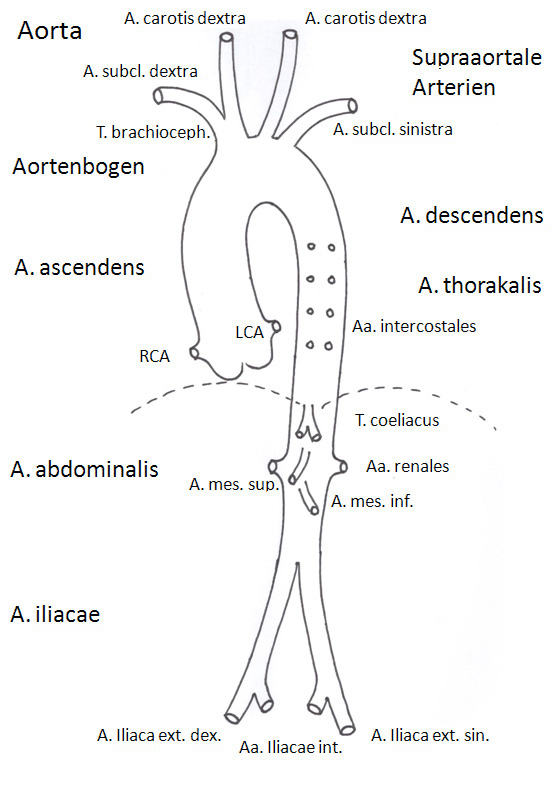
The aorta is the largest artery of the circulatory system, and delivers blood to all of the major organs. It constitutes the main thoroughfare through which the heart pumps blood to the rest of the body (Fig. 1). If the aorta becomes significantly enlarged (aneurysm), immediate action is required. Even in asymptomatic patients, the aorta is at risk of dissection (inner tear) or even rupture once the aneurysm exceeds 5-6cm in diameter. At this size, an aneurysm constitutes an immediate threat to the patient's life. As a result, early detection and preventative surgery to repair the aneurysm are crucial. The risks associated with preventative surgery are significantly lower than those associated with emergency repair.

When an aneurysm is repaired, the affected section is replaced with an artificial vessel (prosthesis). Aortic repair can be performed using conventional open surgery, or by inserting an endovascular stent graft using a catheter-based procedure. Once the aorta has been repaired in this way, the affected section is no longer at risk of dissection or even rupture. Some patients, whose aneurysm is of moderate size, may be able to be treated using a very simple procedure, which involves placing an endovascular stent graft inside the aneurysm. It may be possible for such a procedure to be performed as part of a different surgical procedure, e.g. while a patient is undergoing heart valve replacement surgery for heart valve disease that is associated with an aortic aneurysm.
All aneurysm repairs involving sections of the aorta above the renal arteries are performed using cardiopulmonary bypass (a heart-lung machine). If the aneurysm affects the section of the aorta from which the carotid arteries arise, i.e. if following replacement of this section of the aorta with a prosthesis the carotid arteries have to be reconnected, the heart-lung machine is used to cool the entire body. This effectively places the body in a state of hibernation - allowing the surgeons to work on the carotid arteries without the risk of causing harm to the patient. When dealing with such highly complex procedures, surgeons need to adapt their surgical strategies to suit the individual patient's requirements.
If the aneurysm affects only the ascending part of the aorta, only this isolated section needs to be replaced (Fig. 2). This is a relatively low-risk procedure.
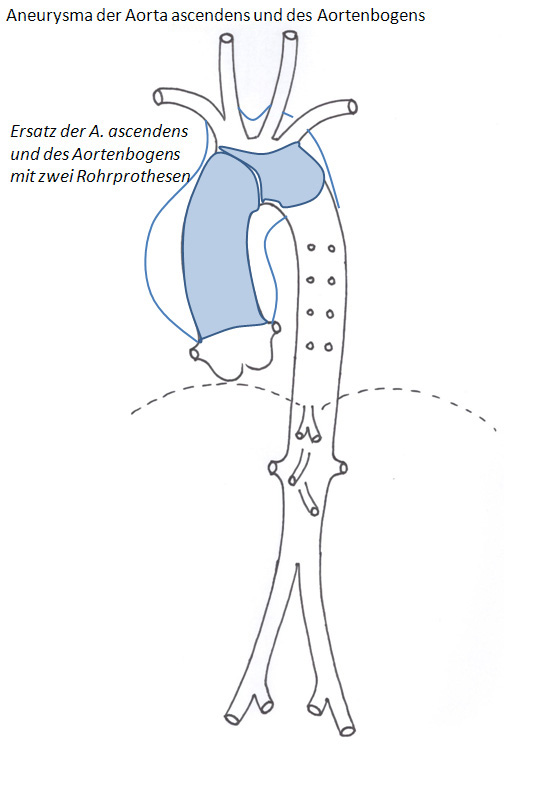
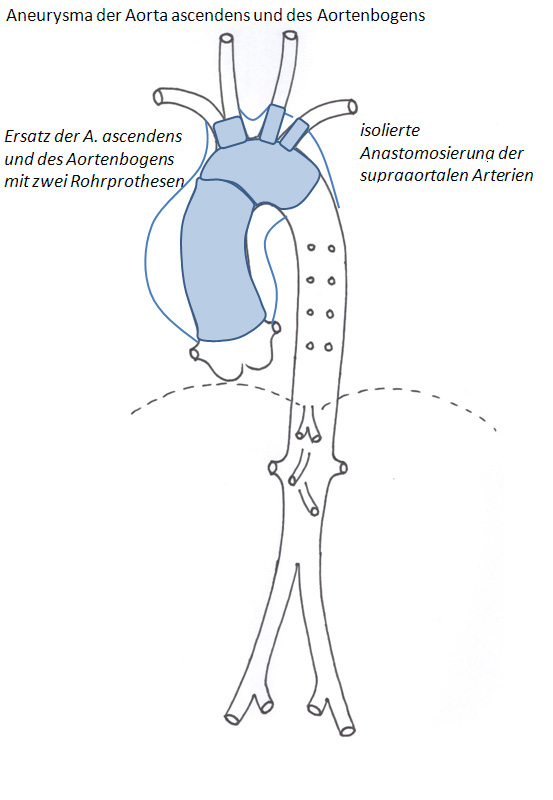
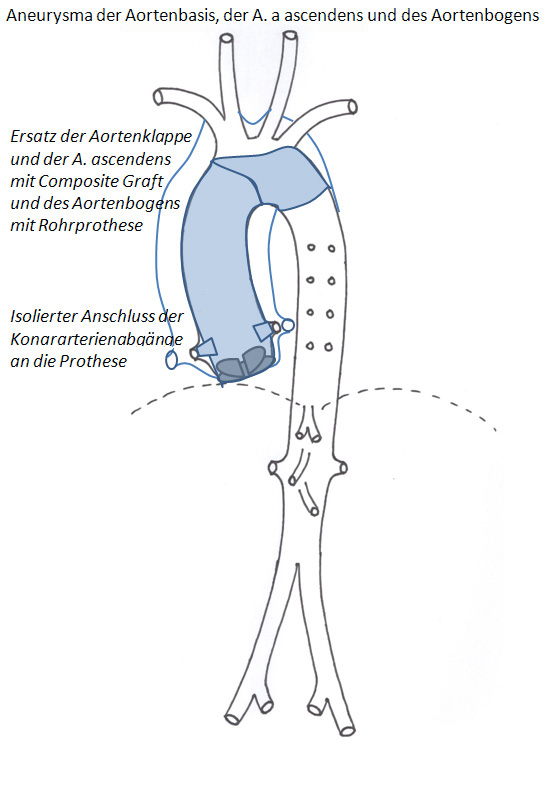
If the aneurysm affects the ascending aorta and the aortic arch, both sections have to be replaced. In order to protect the brain, the procedure to replace the aortic arch is performed using total hypothermic circulatory arrest. If there is involvement of the supra-aortic vessels, these can be reconnected separately. The risks associated with this procedure are higher than those associated with repair of an isolated section of the ascending aorta (Fig. 3, Fig. 4).
What are the techniques used to implant aortic prostheses?
There are two surgical options available for the treatment of aortic disease, open vascular surgery and catheter-based interventions.
Open vascular surgery
Open vascular surgery is usually necessary when the thoracic aneurysm is located in a section of the aorta that is close to the heart (ascending aorta and aortic arch).
If the aneurysm is of moderate size, a simpler type of procedure - which involves placing an endovascular stent graft inside the aneurysm - may suffice. It may even be possible for an endovascular stent graft to be performed as part of a different procedure, e.g. while a patient is undergoing valve replacement surgery.
In most cases, however, it will be necessary to perform prosthetic remodeling of the aorta, a procedure that involves replacing the weakened section of the aorta with a prosthetic tube. As this type of surgery requires an interruption of the blood flow, a heart-lung machine (cardiopulmonary bypass - CPB) is used. Blood returning to the heart is diverted to this machine through a system of tubes. Once inside the machine, the blood is oxygenated before being returned to the body.
If surgery involves the replacement of the section of the aorta from which the carotid artery arises, the CPB machine also cools the blood to 18 degrees Celsius. This slows down the body's metabolism in a way that could be likened to a state of hibernation, thus protecting even the brain against a temporary disruption in the normal blood supply.
Endovascular (catheter-based) surgery
While certain types of thoracic aneurysms are suitable for catheter-based (endovascular) surgical procedures, this type of procedure is particularly useful in patients with abdominal aortic aneurysm. Compared to open surgery, endovascular repair is significantly less invasive, and causes much less trauma to the patient. Endovascular repair involves the physician inserting an endovascular stent graft through an opening in the blood vessels in the groin, and advancing it to the site of the aneurysm. The stent consists of a wire mesh tube covered in synthetic fibers, and is placed inside the aorta in such a way as to effectively exclude the aneurysm from normal blood flow.

The procedure often has to be extended, and the aortic valve replaced as well. This may be because the aortic valve itself is diseased, or because the aneurysm involves the aortic root, making it necessary for the valve to be replaced as well (Fig. 5).
If the aortic valve, the ascending aorta, the aortic arch and the descending thoracic aorta all have to be replaced, this can be achieved using a remarkably refined surgical procedure. As part of this procedure, the aortic arch and the descending thoracic aorta are repaired using what is referred to as a hybrid prosthesis. While the arch of the prosthesis can be likened to a conventional prosthesis, the peripheral section consists of an endovascular stent graft supported by a metal mesh, which is expanded once it has been inserted inside the aneurysm. This approach significantly reduces the considerable risks normally associated with this type of surgery (Fig. 6)
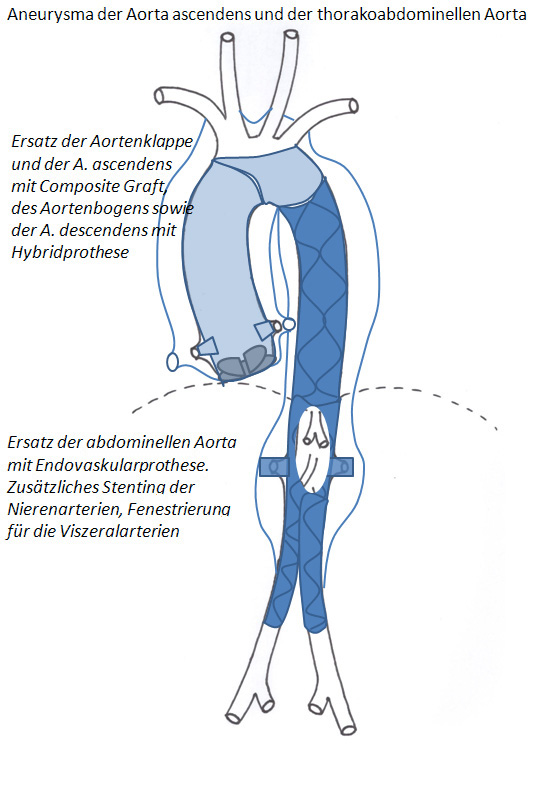
If necessary, an additional endovascular stent graft can be inserted via the femoral artery and attached to the end of the hybrid prosthesis. These endovascular stent grafts are covered in a strong fabric mesh, and ensure that the aneurysm is adequately excluded from the circulation. Naturally, these grafts must leave room for vital arteries to the liver, stomach, intestine and kidneys. For the upper abdominal arteries (celiac trunk, superior mesenteric aorta), this is achieved by using fenestrated stent grafts (stents with the fabric mesh partially removed). For the renal arteries, this is achieved by using individual stent sections. This ensures that, while the aneurysm is excluded, blood flow to the relevant vessels is preserved (Fig. 7).
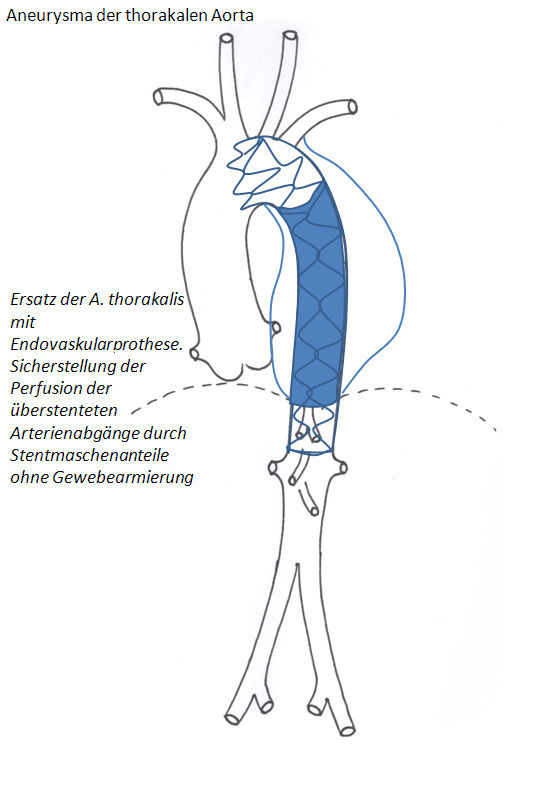
An isolated aneurysm of the thoracic aorta can be treated using a single endovascular stent graft. As this can be inserted using a catheter-based procedure, the patient does not have to undergo complex, open surgery. The prosthetic tube usually needs to be anchored in areas where important blood vessels branch off the aorta, and so it is essential that blood flow to these vessels is preserved (carotid artery, subclavian artery, celiac artery and superior mesenteric artery). For this reason, the end sections of the stent grafts used in these areas are not covered in fabric (bare springs). While the bare springs ensure that the stent is securely anchored and allows blood to flow into the relevant arteries, the covered sections of the stent ensure that the aneurysm is excluded from blood flow (Fig. 8). In terms of risks to the patient, this procedure is much safer than conventional open surgery procedures involving this section of the aorta.
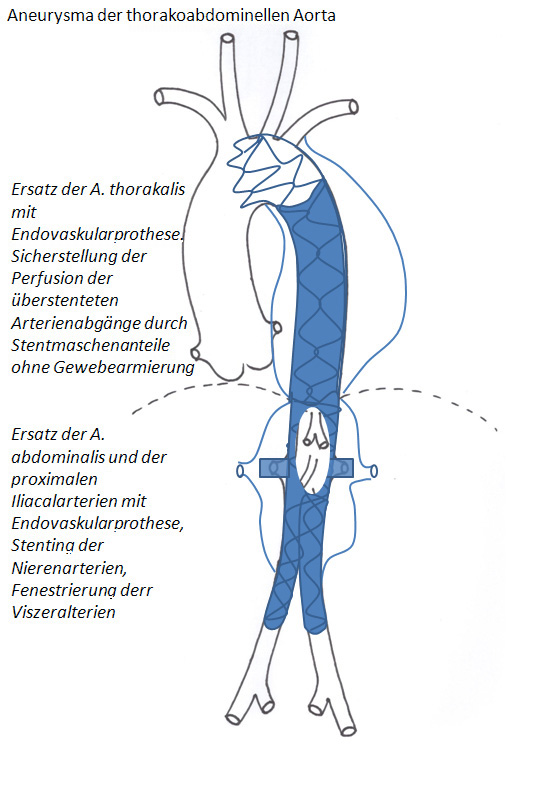
Once again, this procedure also allows for an additional endovascular stent graft to be added to the lower end. This can be done using either custom-tailored openings (fenestrations) or a series of separate stent grafts. (Fig. 9).
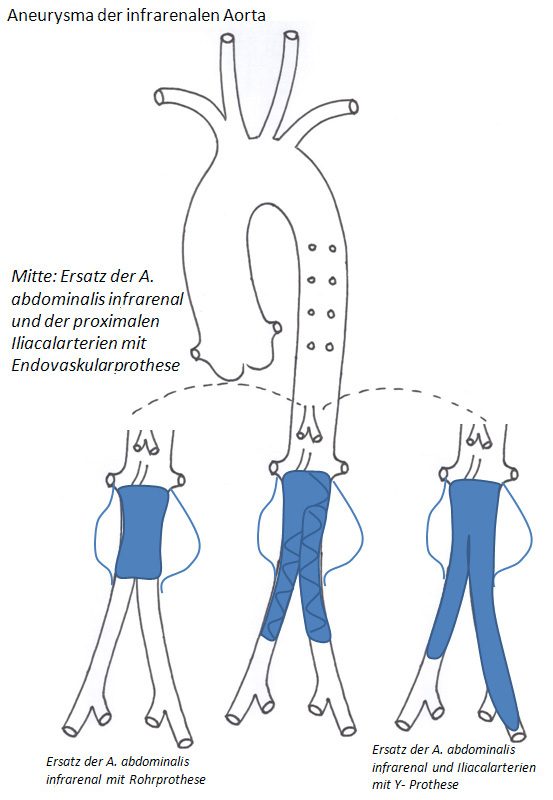
Nowadays, surgical replacement of a section of the abdominal artery below the renal arteries is usually performed using an endovascular stent graft, inserted using a catheter-based procedure. What is significant about this particular procedure is that the prosthesis inserted via the right femoral artery has an opening that eventually receives a smaller prosthesis inserted via the left femoral artery. Once securely linked, these form a Y-shape that ensures blood supply to the pelvis and both of the legs is maintained via the iliac arteries (Fig. 10, middle).
In cases where the insertion of an endovascular stent graft is not possible, the affected section of the abdominal aorta can be replaced in a single open surgery procedure. When compared to catheter-based procedures, the conventional approach places patients at an increased risk. The abdominal aorta and the iliac arteries can also be replaced using a Y-shaped graft, i.e. a bifurcated synthetic stent graft. This involves conventional open surgery (Fig. 10, right).
For most patients requiring the replacement of sections of the ascending aorta and aortic arch, conventional surgery remains the treatment of choice. With regard to patients requiring surgery to replace sections of the thoracic and abdominal aorta, the use of endovascular stent grafts has led to a significant reduction in the surgical risks involved. Here, endovascular repair using a catheter-based approach is the treatment of choice. Aortic aneurysm repair is immensely challenging in terms of the surgical techniques and strategies involved, as well as in terms of the surgical expertise required. This is why such repairs can only be performed at specialist centers, and in close cooperation with cardiology specialists.